-
Primary Endpoint
-
Secondary Endpoint
![Kaplan-Meier Curve of Progression-Free Survival (PFS) for Vectibix + BSC (n=124) and BSC alone (n=119) in patients with wild-type KRAS mCRC.
Proportion of event-free patients from 0 to 100 percent. Treatment duration from 0 to 104 weeks.
In the primary-analysis of PFS, 229 events (disease progression or death) had occurred (115 events in the Vectibix + BSC group [93%]; 114 events in the BSC alone group [96%]). The median PFS for patients in the Vectibix + BSC treatment arm was 12.3 weeks vs. 7.3 weeks in the BSC alone arm.1
Patients in the Vectibix + BSC arm had significant improvement in PFS over those in the BSC alone arm (HR: 0.45, 95% CI: 0.34–0.90 [stratified log-rank P<0.0001]).1](-/media/themes/amgen/amgencompass-ca/amgencompass-vectibix/images/efficacy/group-1.png)
![Kaplan-Meier Curve of Progression-Free Survival (PFS) for Vectibix + BSC (n=124) and BSC alone (n=119) in patients with wild-type KRAS mCRC.
Proportion of event-free patients from 0 to 100 percent. Treatment duration from 0 to 104 weeks.
In the primary-analysis of PFS, 229 events (disease progression or death) had occurred (115 events in the Vectibix + BSC group [93%]; 114 events in the BSC alone group [96%]). The median PFS for patients in the Vectibix + BSC treatment arm was 12.3 weeks vs. 7.3 weeks in the BSC alone arm.1
Patients in the Vectibix + BSC arm had significant improvement in PFS over those in the BSC alone arm (HR: 0.45, 95% CI: 0.34–0.90 [stratified log-rank P<0.0001]).1](-/media/themes/amgen/amgencompass-ca/amgencompass-vectibix/images/efficacy/group-1-mobile.png?h=16&thn=1&w=16&hash=AF262F0989EAE0054C1CF3175B1D24A8)
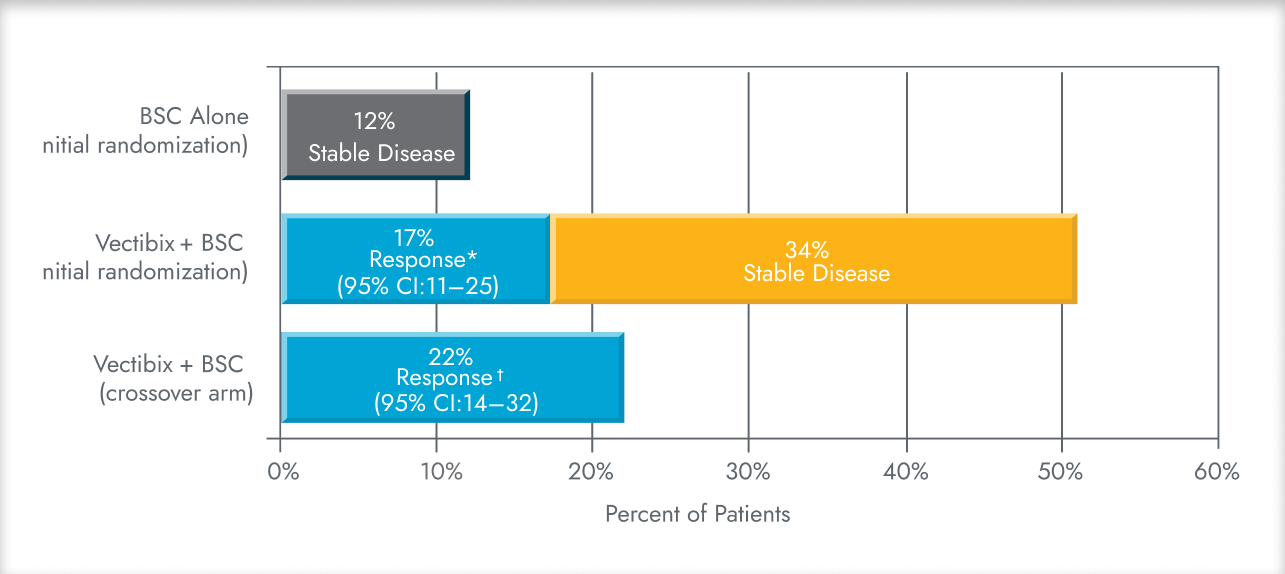
Adapted from the Vectibix Product Monograph1 and Amado et al.4
BSC, best supportive care; CI, confidence interval; HR, hazard ratio; PFS, progression-free survival.

Adapted from the Vectibix Product Monograph1 and Amado et al.4
* Complete response 0/124 + partial response 21/124.4
† Complete response 1/91 + partial response 19/91.4
BSC, best supportive care; CI, confidence interval.

CHARACTERISTICS
All patients (n=463)4,5
| Characteristics | Vectibix + BSC (n=231) | BSC alone (n=232) |
|---|---|---|
| Age | ||
| Mean age (range), years | 61.2 (10.3) | 61.4 (10.8) |
| Gender | ||
| Male (n) | 146 | 148 |
| Female (n) | 85 | 84 |
| Ethnicity | ||
| White (%) | 99 | 98 |
| Primary Tumour Type | ||
| Colon (%) | 66 | 68 |
| Rectal (%) | 34 | 32 |
| All patients (n=463) | ||
| Eastern Cooperative Oncology Group (ECOG) Performance Status | ||
| 0 | 40% | |
| 1 | 45% | |
| 2 | 14% | |
| 3 | 1% | |
| Prior fluoropyrimidine, irinotecan, and oxaliplatin chemotherapy | ||
| 2 lines | 100% | |
| 3 lines | 37% | |
| >3 lines | 6% | |
- ≥18 years old with pathologic diagnosis of metastatic colorectal adenocarcinoma and radiologic documentation of disease progression during or within 6 months following the last administration of fluoropyrimidine, irinotecan, and oxaliplatin.
- Adequate exposure to prior chemotherapy, with average dose-intensity of irinotecan (≥65mg/m2 per week) and of oxaliplatin (≥30mg/m2 per week).
- Two or three prior chemotherapy regimens for metastatic colorectal cancer.
- Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–2.
- ≥1% EGFR-positive membrane staining in evaluated tumour cells (primary or metastatic) by immunohistochemistry.
BSC, best supportive care; ECOG, Eastern Cooperative Oncology Group.
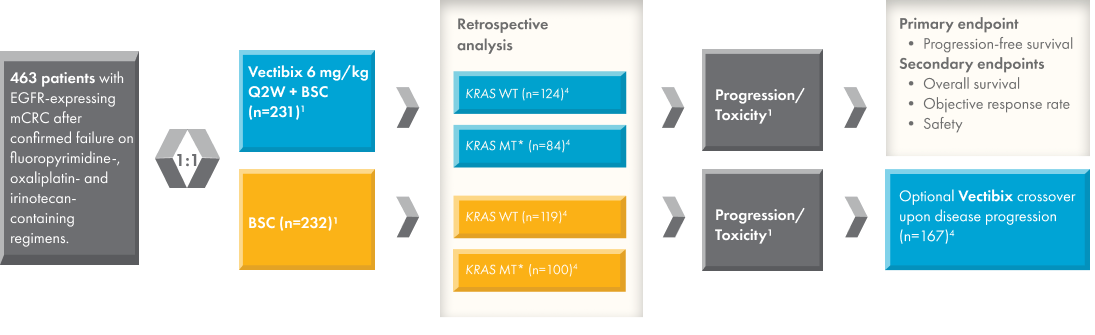

* Vectibix is not indicated for patients with mutant RAS (KRAS/NRAS) or for whom RAS status is unknown.
Adapted from the Vectibix Product Monograph,1 Amado et al.,4 and Van Cutsem et al.5
BSC, best supportive care; EGFR, epidermal growth factor receptor; KRAS, Kirsten rat sarcoma viral oncogene homologue; mCRC, metastatic colorectal cancer; MT, mutant; NRAS, Neuroblastoma RAS viral oncogene homologue; Q2W, every 2 weeks; RAS, Rat sarcoma viral oncogene homologue; WT, wild-type.