-
General management guidelines
A proactive skin regimen should be discussed before Vectibix treatment begins.
Management of dermatologic toxicities requires a multidisciplinary approach, including consultation with nurses, physicians, pharmacists, and other allied healthcare professionals.8,9
When prescribed by a physician, the following skin treatments* may be useful in the management of skin toxicities:1
- Moisturizers
- Sunscreens (SPF >15 UVA and UVB)
- Topical steroid creams (not stronger than 1% hydrocortisone)
- Oral antibiotics (e.g., doxycycline)
Dermatologic and soft tissue toxicity:1
- Clinical manifestations included, but were not limited to, dermatitis acneiform, pruritus, erythema, rash, skin exfoliation, paronychia, dry skin, and skin fissures.
- Patients should be monitored for development of inflammatory or infectious sequelae.
- Life-threatening and fatal infectious complications, including necrotizing fasciitis, abscesses, and/or sepsis, have been observed.
- Stop or discontinue treatment when these complications are severe or life threatening.
- Reported in post-marketing setting: life-threatening and fatal bullous mucocutaneous disease with blisters, erosions, and skin sloughing, including rare cases of Stevens-Johnson syndrome (SJS), skin necrosis, and toxic epidermal necrolysis (TEN).
- In case of the occurrence of SJS or TEN, Vectibix treatment should be discontinued.
* Any treatment decisions are the sole responsibility of the healthcare professional. Please consult the Product Monograph for any treatment option before use. -
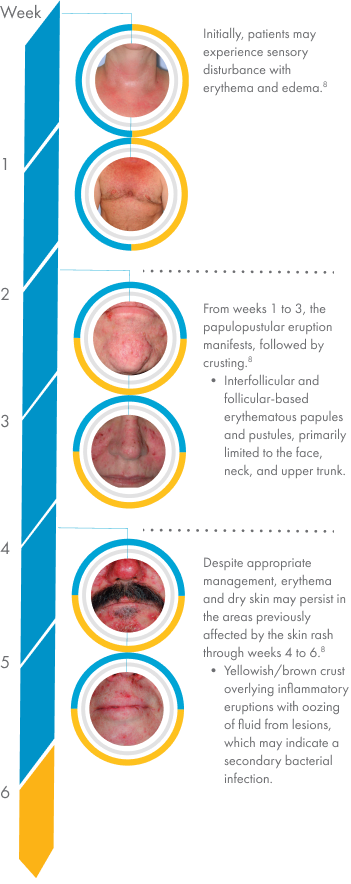
Skin rash
Skin rash timeline
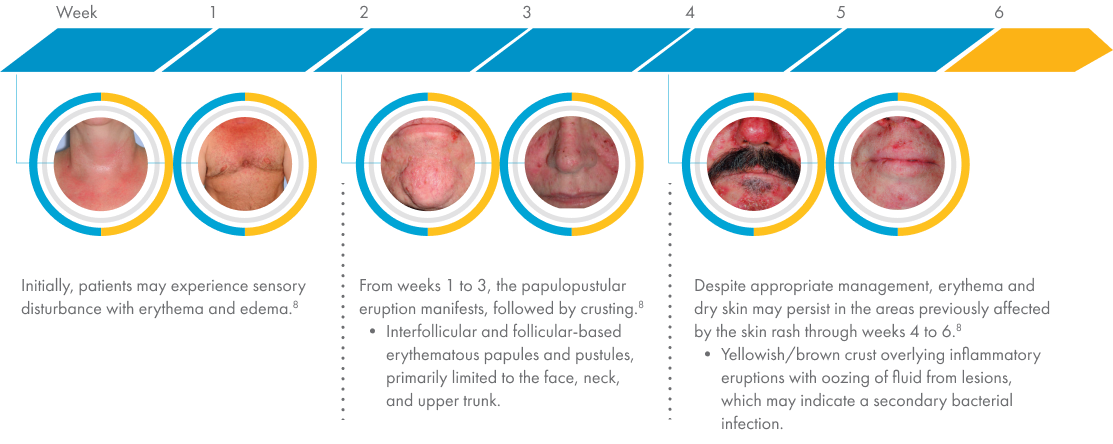
 Patient images may not be representative of the general population. Images: Data on file, Amgen.
Patient images may not be representative of the general population. Images: Data on file, Amgen.
Rash morphology and severity grading



 Patient images may not be representative of the general population.
Patient images may not be representative of the general population.
Images used with permission from B. Melosky.Proactive rash management

Avoid harmful products and/or activities8
Patients should be counselled to avoid activities and skin care products that dry the skin:
- Long, hot showers; saunas
- Alcohol-based or perfumed products
- Over-the-counter acne medication
- Greasy ointments
Sun protection1,8
- Sun exposure can exacerbate rash severity on unprotected areas of the body.
- Patients may be advised to apply sunscreen (SPF >15 UVA and UVB) to their face, hands, feet, neck, back, and chest every morning during treatment.

Protect high-risk areas of the body8,9
- Patients may be advised to moisturize frequently with alcohol-free emollient creams. Applications to the face, hands, feet, neck, back, and chest every morning during treatment are recommended.
- Creams are more effective than lotions, and when kept cool (e.g., refrigerated), they can provide symptomatic benefit.
- Keep nails short and wear protective clothing (e.g., socks and loose-fitting shoes; gloves for housework).
- Liquid bandages may be helpful for sealing fissures or in places where traditional bandages may be awkward (e.g., at the fingertips).
- Consider regular eyelash trimming for patients with elongation or curling of the eyelashes.

Proactive monitoring is key8
- Encouraging patients and helping them manage their side effects is an important part of therapy.
- Teaching patients how to recognize and manage side effects, along with early intervention by healthcare professionals, is necessary.
- Patients should be told to contact their healthcare provider immediately if their side effects worsen.
Reactive rash management1,8
MILD / GRADE 1 MODERATE / GRADE 2 SEVERE / GRADE 3 Mild pustular or papular eruption with few or no symptoms.
Moderate pustular or papular eruption or erythema; moderately symptomatic; may or may not interfere with daily life.
Severe, extensive, painful, intolerable rash; interferes with daily life.

TREATMENT TREATMENT Withhold 1 or 2 doses of Vectibix TOPICAL: Clindamycin 2% + HC 1% in lotion base
Apply BID to affected area until resolution of rashTOPICAL: Clindamycin 2% + HC 1% in lotion base
Apply BID to affected area until improvement of rash by 1 gradeANDORAL:
Minocycline 100 mg PO BIDORDoxycycline 100 mg PO OD to BID
Take for a minimum of 4 weeks and continue for the duration of treatment as long as rash is symptomaticTOPICAL – Scalp lesions:
Clindamycin 2% + triamcinolone acetonide 0.1% in equal parts of propylene glycol and water
Apply lotion until resolutionTREATMENTTOPICAL: Clindamycin 2% + HC 1% in lotion base
Apply BID to affected area until improvement of rash to Grade 1 or 2ANDORAL:
Minocycline 100 mg PO BIDORDoxycycline 100 mg PO OD to BID
Take for a minimum of 4 weeks and continue for the duration of treatment as long as rash is symptomaticTOPICAL – Scalp lesions: Clindamycin powder 2% in amcinonide lotion
Apply BIDImprovement
(< Grade 3)No
ImprovementResume Vectibix treatment according to Product Monograph* Discontinue Vectibix treatment permanently MILD / GRADE 1 Mild pustular or papular eruption with few or no symptoms.
TREATMENT TOPICAL: Clindamycin 2% + HC 1% in lotion base
Apply BID to affected area until resolution of rashMODERATE / GRADE 2 Moderate pustular or papular eruption or erythema; moderately symptomatic; may or may not interfere with daily life.
TREATMENT TOPICAL: Clindamycin 2% + HC 1% in lotion base
Apply BID to affected area until improvement of rash by 1 gradeANDORAL:
Minocycline 100 mg PO BIDORDoxycycline 100 mg PO OD to BID
Take for a minimum of 4 weeks and continue for the duration of treatment as long as rash is symptomaticTOPICAL – Scalp lesions:
Clindamycin 2% + triamcinolone acetonide 0.1% in equal parts of propylene glycol and water
Apply lotion until resolutionSEVERE / GRADE 3 Severe, extensive, painful, intolerable rash; interferes with daily life.
Withhold 1 or 2 doses of Vectibix TREATMENTTOPICAL: Clindamycin 2% + HC 1% in lotion base
Apply BID to affected area until improvement of rash to Grade 1 or 2ANDORAL:
Minocycline 100 mg PO BIDORDoxycycline 100 mg PO OD to BID
Take for a minimum of 4 weeks and continue for the duration of treatment as long as rash is symptomaticTOPICAL – Scalp lesions: Clindamycin powder 2% in amcinonide lotion
Apply BIDImprovement
(< Grade 3)No
ImprovementResume Vectibix treatment according to Product Monograph* Discontinue Vectibix treatment permanently * Refer to the Vectibix Product Monograph for dose modifications related to severe (Grade 3 or higher) dermatologic toxicities.
BID, twice daily; HC, hydrocortisone; OD, once daily; PO, by mouth. -
Proactive and reactive management guidelines for dermatologic reactions
REACTION DESCRIPTION PROACTIVE OPTIONS REACTIVE OPTIONS Dry skin
- Also referred to as xerosis or cutaneous dryness9
- Scaly areas
- In some cases, associated with inflammatory and infectious sequelae1
- Bathing in tepid water with bath oils or mild cleansers9
- Moisturizing creams
- Avoid extreme temperatures and direct sunlight
- Petroleum-based creams; emollients containing urea, colloidal oatmeal9
- Topical zinc oxide (13%–40%); urea creams (10%–40%)
- Topical steroid creams (not stronger than 1% hydrocortisone)
Fissures

- Cracked skin9
- Can be very painful
- Can result from significant xerosis
- In some cases, associated with inflammatory and infectious sequelae1
- Protective footwear and gloves9
- Avoid friction with fingertips, toes, heels
- Thick moisturizers; zinc oxide (13%–40%) creams9
- Wound sealing: cyanoacrylate preparations
- Hydrocolloid dressings; topical antibiotics
- Bleach soaks to prevent infection (1/4 cup of bleach to 3 gal of water)
Paronychia

- Inflammation of the nail folds of the toes and fingers9
- Bleeding
- Significant pain, functional limitation, impairment of activities
- May develop into onycholysis or onychodystrophy
- Diluted bleach soaks (recommended final concentration of approximately 0.005% [1/4–1/8 cup of 6% bleach to 3–5 gal of water])9
- Avoid irritants
- Topical steroid creams (not stronger than 1% hydrocortisone)1
- Systemic tetracycline antibiotics
Pruritus
- Itching sensation9
- Can occur in relation to rash or as a consequence of dry skin
- Gentle skin care9
- Treatment of underlying rash9
- Topical menthol 0.5%; topical pramoxine 1%
- Topical steroid creams (not stronger than 1% hydrocortisone)1
- Systemic antihistamines9
Trichomegaly
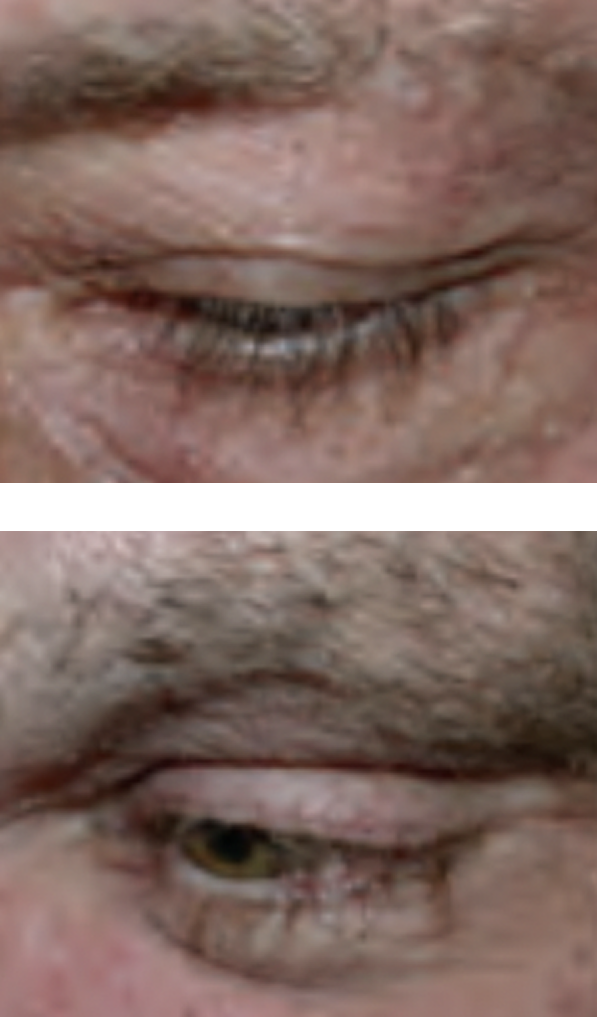
- Elongation and curling of eyelashes9
- Associated with patient discomfort
- Lash clipping every 2–4 weeks9
- Refer to ophthalmologist for irritation or persistent discomfort9
Hypertrichosis
- Increased hair growth anywhere on the body10
- Often presents as facial hirsutism (male-pattern hair growth in women)
Treatment options for womenLaser hair removal plus eflornithine applied to the face and neck9,11
Patient images may not be representative of the general population. Images on file, Amgen (Europe) GmbH. -
Dose modifications for severe dermatologic reactions
For severe (Grade 3 or higher) or intolerable dermatologic toxicities, the following actions are recommended:1
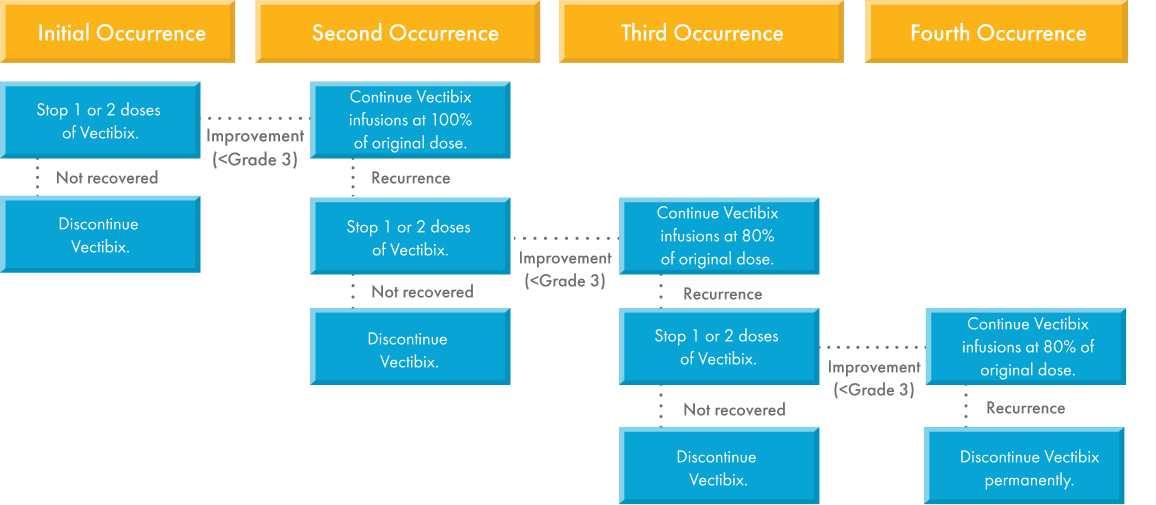
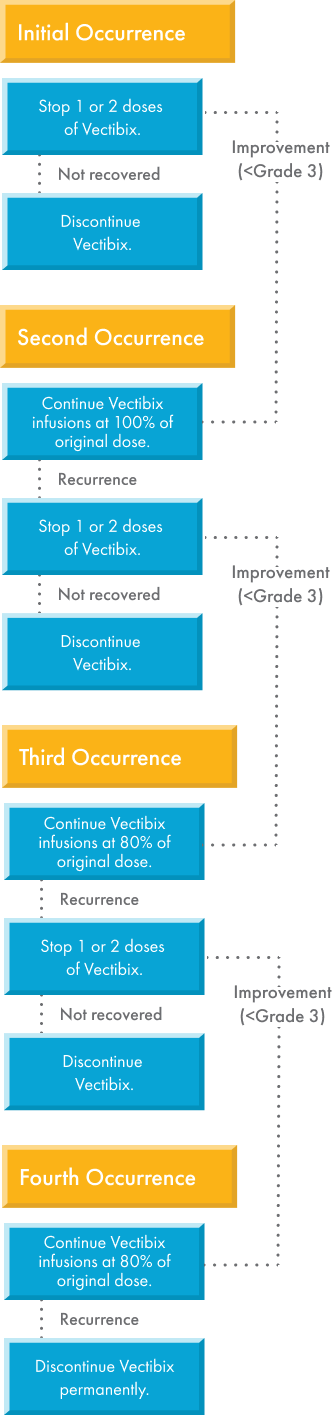
-
Management of hypomagnesemia
Monitoring1
Monitor patients for hypomagnesemia and accompanying hypocalcemia or hypokalemia:
- Prior to initiating Vectibix treatment
- Periodically during treatment
- For up to 8 weeks after completion of Vectibix treatment
Grading12
Grade 1 Grade 2 Grade 3 Grade 4 <LLN–1.2 mg/dL
<1.2–0.9 mg/dL
<0.9–0.7 mg/dL
<0.7 mg/dL
<LLN–0.5 mmol/L
<0.5–0.4 mmol/L
<0.4–0.3 mmol/L
<0.3 mmol/L
Adapted from the National Cancer Institute.13Management
Institute appropriate treatment (e.g., oral or intravenous electrolyte repletion) as needed.
Institutional or provincial recommendations for the management of hypomagnesemia associated with Vectibix treatment may also be available.
LLN, lower limit of normal.
To help you manage treatment of your patients,
skin care sample kits are available.
for more information.